Patients who regain weight after gastric bypass, sleeve gastrectomy, or endoscopic sleeve gastroplasty (ESG) often arrive at clinic feeling discouraged, and sometimes ashamed. That response is understandable, but it does not reflect personal failure. Obesity is a chronic medical condition. The body is wired to defend energy stores, and weight recurrence after any intervention is a recognized part of long-term disease biology.
Dr. Kalpit Devani, an interventional gastroenterologist in Greenville, South Carolina, helps patients reinterpret regain as a signal to reassess treatment, not as evidence that prior care "did not work."
Why Weight Comes Back
No single procedure produces permanent weight loss for every patient. Bariatric and endoscopic interventions create a powerful window of reduced intake, improved satiety, and metabolic change. For many people, that window lasts years and delivers meaningful improvements in blood pressure, diabetes, sleep apnea, joint symptoms, and overall longevity.
Over time, anatomical changes (such as pouch or outlet dilation), hormonal adaptation, medication changes, stress, sleep disruption, and gradual dietary drift can allow weight to return. This pattern is expected in chronic disease management, not unique to one operation or one individual.
Reframing "Failure"
Labeling a patient or a procedure as a failure oversimplifies obesity care. A gastric bypass that supports substantial weight loss and remission of type 2 diabetes for a decade has already improved health, even if some weight returns later. The clinical goal is to extend periods of better metabolic health and to intervene early when weight trends upward.
Shame discourages people from seeking help. In practice, the most productive next step is a structured evaluation: current weight trajectory, eating patterns, activity, medications, prior operative or endoscopic anatomy, and comorbidity status.
Options When Weight Regains
Treatment is not one-size-fits-all. Depending on history and anatomy, options may include:
- Intensified lifestyle and nutrition support with a registered dietitian and behavioral counseling
- Anti-obesity medications, which can be layered onto prior surgical or endoscopic treatment when appropriate
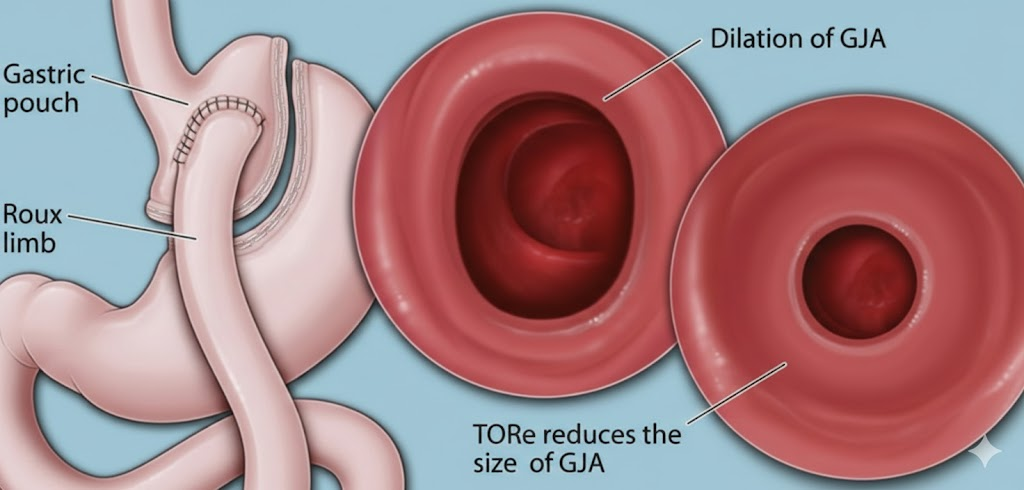
- Endoscopic revision for selected post-bypass patients with a dilated gastrojejunal anastomosis, [Transoral Outlet Reduction (TORe)](/blog/transoral-outlet-reduction-tore) narrows the outlet endoscopically without repeat abdominal surgery
- Repeat or alternative procedural approaches when anatomy, goals, and prior interventions support further care
Some patients require more than one intervention across a lifetime. That is consistent with how other chronic diseases, hypertension, asthma, inflammatory bowel disease, are managed over decades.
When to Seek Evaluation
Consider specialty review if you have regained a significant portion of lost weight, if comorbidities are worsening again, or if you are unsure whether anatomical dilation may be contributing. Endoscopic assessment can clarify whether revision procedures such as TORe are reasonable.
Patients in the Upstate region can explore endoscopic weight loss options and TORe for post-bypass regain with Dr. Devani. Early conversation prevents years of silent frustration and opens the door to evidence-based next steps.
Frequently Asked Questions
Is weight regain after bariatric surgery normal?
It is common. Obesity is chronic, and the body adapts over time. Regain does not mean the original procedure had no value or that the patient lacked willpower.
Does weight regain mean my surgery failed?
Not necessarily. Many procedures deliver years of improved weight and health. Regain often reflects disease recurrence and may respond to additional treatment.
What is TORe and who might need it?
Transoral Outlet Reduction is an endoscopic revision that tightens a dilated gastric outlet after Roux-en-Y gastric bypass. It may help selected patients with anatomic dilation and weight regain.
Can medications help after regain?
Yes. Modern anti-obesity medications can be combined with prior surgical or endoscopic treatment when clinically appropriate, as part of a comprehensive long-term plan.
Dr. Kalpit Devani, MD, FACP, FACG, FASGE is a board-certified interventional gastroenterologist based in Greenville, South Carolina, specializing in diagnostic and therapeutic EUS, complex ERCP, and endoscopic suturing.
Related Posts
Five Common Misconceptions About Endoscopic Sleeve Gastroplasty (ESG)
Misinformation about endoscopic sleeve gastroplasty persists online. Here are five myths patients often hear, and what the evidence actually shows about safety, durability, and candidacy.
Read more →Colon Cancer Screening: When to Start, What to Expect, and Why Early Detection Saves Lives
Colon cancer is preventable with timely screening. Learn when to start, what happens during a colonoscopy, and why early detection saves lives.
Read more →Life After ESG: What to Expect in the First Year After Endoscopic Sleeve Gastroplasty
What happens after Endoscopic Sleeve Gastroplasty? Learn about the recovery timeline, diet progression, expected weight loss, and long-term success.
Read more →This article is for educational purposes only and does not constitute medical advice. Please consult your physician for individualized care.