Overview
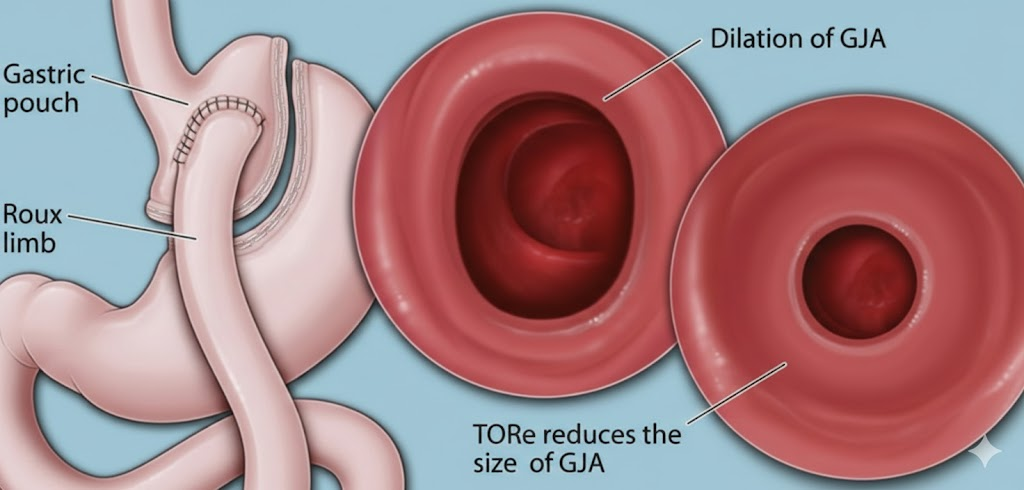
Roux-en-Y gastric bypass remains one of the most effective operations for sustained weight loss and metabolic improvement. However, a subset of patients experiences weight regain years after surgery. Dilatation of the gastrojejunal anastomosis (the connection between the stomach pouch and the small intestine) is a recognized contributor. When the outlet widens, more food passes through before satiety signals are triggered, undermining long-term weight maintenance.
Transoral Outlet Reduction (TORe) is a minimally invasive, incision-free endoscopic procedure that reduces the diameter of the dilated gastrojejunal anastomosis. Performed entirely through the mouth using advanced suturing technology, TORe offers selected patients a non-surgical revision option without the risks and recovery burden of repeat bariatric surgery.
What Is TORe?
TORe is performed using a flexible endoscope advanced through the mouth into the stomach pouch. The physician visualizes the gastrojejunal anastomosis (the outlet created during the original gastric bypass) and uses endoscopic suturing to place folds around its circumference. These sutures reduce the outlet diameter, restoring a smaller opening that promotes earlier satiety and limits food intake.
Key procedural points:
- No external incisions, everything is done endoscopically through the mouth
- No tissue removal, the outlet is narrowed with sutures, not resected
- No surgical stapling, sutures create the new contour
The procedure is performed under sedation. Most patients are discharged the same day.
How TORe Works
During gastric bypass, the stomach is divided into a small pouch and a larger remnant. The pouch connects to the small intestine through the gastrojejunal anastomosis. Over time, this opening can stretch and widen, allowing larger volumes of food to pass before the patient feels full.
TORe addresses this by reducing the outlet diameter through endoscopic suturing, creating plications that narrow the anastomotic opening and restore a more restrictive configuration, similar to the immediate post-bypass state. The goal is to re-establish early satiety and support weight loss or weight stabilization when combined with lifestyle modification.
Benefits of TORe
TORe offers several advantages for appropriately selected patients:
- Minimally invasive and incision-free: avoids the risks of repeat open or laparoscopic surgery
- Outpatient procedure: typically no hospitalization required; most patients go home the same day
- Faster recovery: return to normal activities within one to two weeks, versus weeks to months with revisional surgery
- Reduced surgical risk: no abdominal incisions, wound complications, or longer hospital stay
- Meaningful weight loss potential: when combined with structured follow-up and lifestyle modification, TORe has been associated with weight loss or stabilization in appropriately selected patients with a dilated anastomosis
Who May Benefit?
TORe may be appropriate for patients who have undergone Roux-en-Y gastric bypass, are experiencing weight regain (typically with a dilated gastrojejunal anastomosis confirmed on imaging or endoscopy) and prefer a non-surgical revision approach. Candidates should be motivated to resume or intensify lifestyle and dietary changes.
Careful evaluation is essential. Endoscopy, imaging, and assessment of anatomy and motivation help determine whether TORe is the right option. Not all patients with weight regain are candidates.
Procedure and Recovery
TORe is performed under conscious sedation or general anesthesia. The procedure typically takes 45-90 minutes. Patients are monitored in recovery and usually discharged the same day.
Post-procedure diet advancement is staged, similar to the early post-bypass period. Detailed dietary instructions protect the revised outlet and support healing. Long-term success depends on adherence to dietary guidelines and ongoing lifestyle support.
Outcomes and Follow-Up
Outcomes vary with patient selection, technical success, and commitment to lifestyle modification. Careful endoscopic and sometimes radiographic evaluation helps identify patients most likely to benefit. Long-term follow-up, including nutrition support and behavioral counseling, is recommended to optimize results.
Dr. Kalpit Devani, MD, FACP, FACG, FASGE is a board-certified interventional gastroenterologist based in Greenville, South Carolina, specializing in diagnostic and therapeutic EUS, complex ERCP, and endoscopic suturing.
Related Posts
Five Common Misconceptions About Endoscopic Sleeve Gastroplasty (ESG)
Misinformation about endoscopic sleeve gastroplasty persists online. Here are five myths patients often hear, and what the evidence actually shows about safety, durability, and candidacy.
Read more →Weight Regain After Bariatric or Endoscopic Weight Loss: What It Means and What You Can Do
Regaining weight years after bariatric or endoscopic weight loss is common, and it is not a moral or personal failure. Obesity is a chronic condition that often requires ongoing treatment.
Read more →Colon Cancer Screening: When to Start, What to Expect, and Why Early Detection Saves Lives
Colon cancer is preventable with timely screening. Learn when to start, what happens during a colonoscopy, and why early detection saves lives.
Read more →This article is for educational purposes only and does not constitute medical advice. Please consult your physician for individualized care.